Introduction
Originating from a concern on the linkage between health policies and immigration policies within healthcare organizations, our goal is to understand how and why healthcare organizations adapt their services to the needs and characteristics of migrant populations: while the dynamics of migratory processes are well documented, organizations’ ability to adapt is not1,2. This is the challenge, we wish to address.
In doing so, we used three angles of analysis: (1) interactions between the stakeholders within an organization viewed as a Complex Adaptive System (CAS), especially between an organization’s various levels of governance; (2) the levers of action implemented by the multiple stakeholders; and (3) the factors that influence the stakeholders.
We propose a conceptual model of multilevel adaptive governance able to reconcile two paradoxical adaptation mechanisms: (1) multiple autonomous stakeholders are able to self-organize while acting in a heterogeneous manner; (2) governance allows these heterogeneous actions, through levers of action, to converge toward a more homogeneous collective process. To develop this framework, we rely on the theories of complexity and governance.
Why adapt services to migrant populations?
In industrialized countries, migrant populations experience a deterioration of their health, despite access to a universal health care system and a better health status than non-migrants upon arrival3. There are differences in the degrees of vulnerability to which migrants are associated4. In this article, we adhere to the definition of vulnerable populations by Frohlich and Potvin: “a vulnerable population is a subpopulation who, because of shared social characteristics, is at a higher risk of risks”5. Although not all migrants are vulnerable, many share numerous social characteristics that put them “at risk”; this includes socioeconomic instability, isolation from their families, mental health and depression taboos, and language barriers6,7.
Immigration in and around large urban centers has left health professionals facing important issues in matching services to the needs of these new populations8. Because this challenge was not anticipated, professionals must intervene as “experts” on a case-by-case basis. Under these circumstances, the self-organization of each individual stakeholder comes into play.
Our goal is to illustrate, through the theories of complexity and governance, the issues posed by the adaptation of healthcare organizations to migrant populations’ needs.
The Healthcare organization as a complex adaptive system (CAS)
Organizations are composed of multiple interdependent stakeholders driven by their own interests9. They are the sites of numerous power plays and power relationships. From a complexity perspective, tensions and conflicts can provide fertile ground for tangible agreements between stakeholders, depending on the degree of connectivity that exists between them10,11. As per the theories of complexity, this vision and the concept of “fractal organization” may be brought together: each part of the organization mimics the organization as a whole; the structure repeats itself at various levels, and the organization found at each level is the same as that of the organization as a whole12,13,14. In addition to links that can unite certain stakeholders within a complex organization, the fractal character of this organization can multiply the interactions 15 and reduce the rigidity of the organization’s hierarchy16,17.
According to Begun and Zimmerman18 , healthcare organizations are an ideal ground for applying the sciences of complexity and CAS. Additionally, they are seen as dynamic and almost continually evolving due to medical, technological, demographic, socioeconomic, and political advances.
In this section, we define three processes of CAS: self-organization, self-eco-organization, and co-evolution. We will refer to these definitions to develop our conceptual framework.
Self-organization
Self-organization is stakeholders’ capacity to autonomously adapt. The mechanism of self-organization highlights stakeholders’ ability to be creative and innovative. They are “diverse agents that learn”19.
Self-organization is the individuals’ adjustment with respect to the interactions that he or she has with the other stakeholders in an organization. These actions are made possible by schemata, the personal interest of the stakeholder, and his or her connections with the local context9. Shemata is “a cognitive structure that determines what action the agent takes at time, t, given its perception of the environment”9:219. We consider the schemata as individual and heterogeneous in the process of self-organization.
Positive and negative feedbacks also facilitate self-organization9,64. Positive feedback allows stakeholders to continue in the direction of the action undertaken. It may originate from unexpected changes due to certain interactions20. By contrast, Negative feedback consists of a return to initial conditions in which the effects of adaptation and change are diminished.
Self-organizations depend on each individual stakeholder within the organization, which means that the possible behaviors may be heterogeneous. Self-organization often appears to be improvised and spontaneous21, not imposed by hierarchy. As stakeholders become accustomed to working together, they may adopt a shared global vision, and share their experiences and expertise. However, in the long term, the adaptation process may stop at that level and not be extended to the rest of the organization. Positive feedback can be manifested at the individual level and in a heterogeneous way; however, at the organizational level, the lack of organizational support may prevent knowledge and experience capitalization by the whole organization22.
Conversely, a healthcare organization that supports the innovations of its personnel can easily capitalize on the adaptation processes that take place in one of its departments. The expected effect is that of a snowball, in which all trials-and-errors successes are complementary while remaining interlinked within the context and the specificity of each case. The principle of positive feedback is applicable in this scenario, as the change implemented at time t1 continues its progress toward times t2, t2bis, t2ter, etc. without going back to time t0.
Self-Eco-organization
Self-eco-organization is the ability of each stakeholder to adapt while interacting with the Environment23. When the adaptation process is seen by the organization as an important issue, internal and external stakeholders at the clinical and administrative levels are encouraged to work together: they self-eco-organize by generating more interactions and more interdependence within the organization and the Environment. Achieving a better service integration requires re-centering the autonomy of each involved entity to facilitate the creation, extension, and evolution of the interactions. Based on our reading of CAS, self-eco-organization is the cornerstone of integration from which “manipulations of interdependences” emerge among the various stakeholders in a system24. The result is an improved coherence between the organization and the Environment. As per Nonaka25, the formation of “self-organizing teams” facilitates trust between stakeholders thus accelerating the knowledge and experiences exchange with regards to service adaptation.
Co-evolution
However, the organization adapts to its Environment in a dual relationship26. Co-evolution is the aggregate of the self-eco-organization of the healthcare organization and the Environment: it is the interaction point between the internal and the external. Co-evolution refers to the interdependent relationship between the organization and its Environment. Different stakeholders, linked together, share a vision and act towards the same goal: adapting services to a subgroup presenting its own specificities.
The Environments’ response to a “stimulus” from the organization can alter both the organization and the Environment27. The organization acts and reacts in a cooperative or competitive manner with the stakeholders of the Environment. In turn, the stakeholders from the Environment (who also have other types of self-eco-organization) are influenced and influence those of the organization28. This process involves mutual adaptation. The process of co-evolution between the organization and the Environment can allow, for example, certain forms of shared leadership to develop29. This may lead to tensions, often due to unbalanced relationships of power between the multiple stakeholders30.
The nature of governance in healthcare organizations
To understand the adaptation process, healthcare organizations have developed different ways of collaborating with each other. Their nature varies depending on whether the organizations find themselves in the clinical or administrative sphere.
Adaptation in a complex healthcare organization
Adaptation refers to the ability to act and react to changes in the Environment27. To relieve tensions, particularly in relation to diversity, the adaptive character of the system is fundamental28,31,32.
According to Moore and Kraatz, adaptation is a paradoxical phenomenon that requires “novelty, variation, risk taking and a diversity of perspective” as well as “constancy, homogeneity, shared identity and common purpose”33:16. Miller and Sage make an interesting distinction between two forms of adaptation: heterogeneous and homogeneous31:102. Depending on the levels of adaptation required, ranging from heterogeneous to extremely homogeneous, the behaviors of the stakeholders, and of the system as a whole, are influenced by operating rules that are dependent on the context and the final interests at stake27.
Heterogeneous adaptation is the adaptation of a stakeholder oriented by his or her own interests and the satisfaction of his or her needs without necessarily taking into consideration the adaptation of the other stakeholders. In the case of adaptations to new challenges that must proceed through various fields and spheres of an organization, heterogeneous adaptations may become barriers to the coherence of the actions. Interdependence between stakeholders should thus be encouraged.
If healthcare organizations give priority to service adaptation, stakeholders should be moving in the same direction, thus creating “Migrant Friendly” organizations34. For that reason, the term “homogeneous adaptation” is used: not to reduce autonomy or individual freedom but rather to maximize the collective coherence and the quality of care and services.
Governance of complex healthcare organizations
By integrating the above-discussed concepts, governance becomes a tool for self-eco-organization, stimulating homogeneous adaptation. This tool allows for the preparation of internal policies through the collaboration of multiple stakeholders. The goal is to maintain collective coherence between the internal stakeholders and the Environment stakeholders: co-evolution, a shared vision: schemata, and consequently a dynamic and emergent structure for the organization: self-eco-organization.
The conceptualization of governance according to a complex perspective questions the distribution and the future of the organizations’ authority and power35. In fact, “the stronger the uncertainty, the more difficult it is to program and routinize action in planning what should be done”35:86. The organization is then defined by features other than control mechanisms. It will focus more on the goals to be achieved rather than on how to achieve them thus allowing free rein for creation and innovation to achieve those goals. A structure with more permeable borders is put into place, allowing transformations to guide stakeholders towards a self-eco-organization while maintaining specific goals to be attained through co-evolution. Stakeholder influence is not definitive and can vary in its duration and intensity. Dubinskas calls this phenomenon “coupling”, in which pairs of stakeholders form, and these pairs can exert close (tight) or distant (loose)37:363-364. Depending on the degree of influence or coupling exercised, it is possible to move towards an organization that is capable, collectively, not only of giving value to what it has acquired i.e. exploitation, but also of allowing innovation to emerge via exploration37.
Multilevel governance within complex healthcare organizations
According to 38, the term “multilevel governance” emerged in the 1990s and was applied in a manner extensible to the political domain. Multilevel governance can occur at different scales (organizational, territorial, and societal) and involves stakeholders coming from different structures who interact with each other38. Multilevel governance then becomes, through the processes of self-eco-organization and co-evolution, the focal point that can link four worlds, “cure, care, control and community”, as highlighted in39,40,41. In our study, cure represents the medical community and the biomedical activities associated with it. Care is more inherently linked to the activities of nurses, other non-medical professionals, and community workers. Control is the sphere of “bureaucratic” or traditional administration. Finally, community represents the persons linked directly or indirectly to the healthcare organization (such as community groups, interest or influence groups, and members of the government or local politics).
In a primary care organization, two spheres coexist: clinical and administrative. The clinical sphere is concerned with phenomena linked to the clinic and to the professionals and manages the interface with the administrative sphere. It primarily focuses on cure, care and community, while accommodating control from the managers. The administrative sphere manages organizational phenomena in alignment with the clinical sphere, which it serves, and not the converse42.
The levers of action in multilevel governance
Some levers of actions exist in both spheres: this is the schemata9. As seen previously, the schemata is individual and heterogeneous in the process of self-organization and it can be shared by various stakeholders, who may make it collective (either at the scale of a service or applied to the entire organization). The collective schemata then influences the individual schemata (the schemata of health professionals, other employees, administrators, and others). In unifying itself around a clear and defined position with respect to the need to adapt its services, the organization takes an important role in collective action and in the governance of the adaptation process. For this reason, the official position and internal policies should be clear and coherent43,44,45.
At the structures level, it is the role and functions of each stakeholders, depending on the type of management and governance established that prevail. Depending on the choices made, it is possible for stakeholders of the administrative sphere to support, validate, and legitimatize actions undertaken in the adaptation process. This obviously does not always occur.
At the level of politics, the existence, knowledge, and implementation of principles, norms, and explicit rules regarding the adaptation of health services are important. In particular, the clinical sphere puts forward functional and clinical integrations46,47. The desired vision of the establishment, in terms of normative integration, leadership, coordination, and communication, is put forth by the administrative sphere46,48.
There are three principal resources. Human resources comprise professionals focusing on health, training, and education regarding best practices; tools assisting with decision-making; and the use of guides for interventions and approved protocols for care. These resources focus on the particular staff deployed to deliver the adapted services49. Financial resources refer to the priority given to service needs in the area of care for migrant population, while accounting for internal and external constraints. Finally, temporal resources designate the accounting, by clinical and administrative managers, of the supplementary time necessary for professionals to self-eco-organize to evaluate, orient, and follow-up with migrant patients8.
Knowledge levers focus on training, education best practices, the development of tools to support decision making and the use of intervention guides and evidence-based care protocols.
Communication and informational levers refer to publicity and promotion mechanisms, such as a group of interpreters, instructional material adapted and translated, and similar types of potential outreach65. In the administrative sphere, this resource type refers to measures implemented to collect information (including indicators, evaluations, and results) and to inform stakeholders on the types of clients served and the different clinical adaptations offered by the establishment.
The influence factors of multilevel governance
Depending on the degree of coupling, the healthcare organization acts and reacts in a continuous way to multiple internal and external factors. We identified four types of factors of influence:
Cultural factors concern the perception of adaptation and the associated values, particularly with regards to immigration. As a lever of action, schemata can have an impact depending on the understanding that stakeholders have of health services: health services solely considered from the perspective of their efficiency in solving a health issue retain little space for adaptation in the long term. Conversely, from the viewpoint of efficiency and the perspective of their acceptability to those who receive them, health services retain more space for adaptation;
Clinical factors address the degree of autonomy of the clinical stakeholders, notions of leadership, case assignment based on human resource availability and interest, and the roles of the various professional corps in the decision-making process;
Organizational factors concern the prioritization of service adaptation within the administrative lines of direction, assigning dedicated resources while accounting for cost, time, information, budgetary restrictions;
Contextual factors are numerous and refer to pressures from the Environment (NGOs, ministers, citizens) that may (inter)act within the various governance levels, and influence the adaptation process.
These four types of factors are interdependent and act simultaneously on the interactions between the stakeholders of the organization and the Environment. The power struggles and the degrees of coupling will negatively or positively accentuate the impact of these factors and will likewise contribute to the relative equilibrium or instability of the adaptation process50.
Definitions and representation of the multiple levels of governance
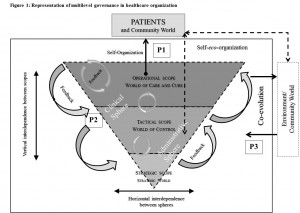
The convergence of these levers and factors is possible when a governance structure exists at multiple levels in the organization and influences both the schemata and the interests of the internal and external stakeholders. Multilevel governance is then divided into three fields of action: operational, tactical, and strategic51 (Fig.1).
In accordance with Figure 1:
The operational field of action represents the group of frontline professionals involved in clinical practice with patients, i.e. “all processes involved in the care for clients, in which an inherent uncertainty requiring professional judgment exists”52:170.
The tactical field of action relates to management stakeholders. This field is responsible for translating strategic directions to the operational level and commissioning reports of actions undertaken at the operational level to the strategic level. It allows the establishment to self-eco-organize, acting as the junction point between the heterogeneous self-organization of the multiple stakeholders of the organization and the Environment.
The strategic field of action represents the “hierarchical” space for decision-making, i.e., the upper echelons of the establishment (General Director, director of nursing care, etc.) Part of its role in the multilevel governance is to assemble and maintain collective schemata that is coherent, integrative and homogeneous for the administrative and clinical spheres, while accentuating co-evolution with the Environment.
Representation?of?multi-level?governance?in?a?healthcare?organization
{kind=link}
Consequently, the governance of a complex healthcare organization is a tool of self-eco-organization (Fig. 1). It addresses the specific needs of each sphere (clinical and administrative). It respects the autonomy of the stakeholders and, at the same time, facilitates, through feedback, internal interdependences between the operational, tactical, and strategic fields.
Governances’ instrumentation within a complex organization allows the set of heterogeneities to become homogeneous, facilitating the convergence of adaptation measures. The development of multilevel governance allows the whole activity to be re-centered, avoiding isolated, non-integrated and non-recursive actions, thus facilitating the adaptation process.
Stakeholder participation in the adaptation process is facilitated by emergent mechanisms that seek to let the voices and ideas of operational and tactical stakeholders be heard by strategic stakeholders. Thus, the adaptation process through multilevel governance allows the organization to become “fractal”, and regardless of its scale, the adaptation process takes place in a similar fashion. Through the interactions between stakeholders, similar behaviors and rules influencing them will be found, regardless of the sphere in which they interact, which will guarantee a certain organizational stability53. Multilevel governance can be a mechanism through which adaptation is generalized to the entire organization. In other words, we postulate that, in addition to observing that a complex organization can have fractal characteristics54,16,20,38,55,56, it is possible to deliberately fractalize it with the help of the multilevel mechanism involved in the governance. This process grants more space for professionals in the clinical sphere when it comes to developing collective actions and decision-making57,25.
Multilevel adaptive governance: a space for coherence for multiple stakeholders in multiple spheres
According to Lamothe (2007), a governance that allows adaptation favors realistic leadership. According to the author, “the adaptation of the structural-administrative framework emerges equally from a learning process subject to the combined influence of inter-professional and inter-organizational dynamics”57:296. Through the creation of social and health services networks, such as those implemented in Québec, the change should operate in a horizontal way and generate a detachment from bureaucratic management modes in favor of closer modes of cooperation with professionals achieved by involving them directly in the change process29.
According to 58, adaptive governance involves a transfer of decisional power from managers to a broader participative level among the various services. This co-management is not automatic, and most often, it self-eco-organizes in a social network made up of teams and groups of stakeholders representing these different services to create spaces for deliberation and decision-making. This type of network includes stakeholders from the Environment (community organisms, municipalities, and the other previously discussed entities), and through this path a co-evolution emerges.
However, without Generative Relationships, there can be no co-evolution or adaptation…
Stroebel26, following Abbotts’ studies59, invites us to change our conception of healthcare organizations, moving away from considering these organizations as entities functioning linearly, experiencing unique events and engaging in processes that are not interlinked, to a way of thinking based on the following terms: ‘patterns, interrelated processes and relationships’26:440. This conception of the relationships between stakeholders is also shared by Lane and Maxfield, who call these associations ‘generative relationships’60:216:
[that] induce changes in the way the participants see the world and act in it and even give rise to new entities.
Thus, in an unstable and unpredictable context, various stakeholders can learn and co-create new models, new schemata and new solutions61. Establishing connections and networking with stakeholders from the Environment influences and encourages the healthcare organization to adapt its services to various subgroups of populations. At the same time, the generative relationships, internal and external to the organization, become both levers of action and factors of influence, primarily in terms of co-evolution. This function allows for emphasis to be placed on the need to adapt health services for all of the stakeholders involved in multilevel governance.
Based on the studies reported in 57,58, we propose the novel term of multilevel adaptive governance.Multilevel adaptive governance allows healthcare organizations, within a given context, to grasp the breadth of the migration question. The organization becomes a space within which the voices of stakeholders from the operational field benefit from the credibility of the tactical and strategic fields. Conversely, administrators from the strategic field have a continual need for legitimacy on the part of stakeholders from the other fields, and particularly from health professionals. Thus, a coherent language is developed through communication, comprehension, and action between the two spheres and the three fields; this helps refine the adaptation process, and connect it explicitly with the vulnerability of the populations served62,63.
The conceptual framework of the process of adaptation of multilevel adaptive governance: Several proposals concerning healthcare organizations
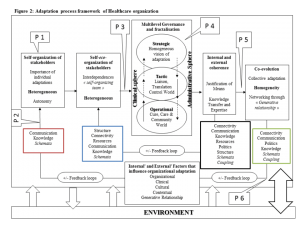
In part 1, we selected certain concepts from CAS to describe healthcare organizations. Then, in part 2, we defined the concepts of multilevel governance and adaptation, to link them in part 3 with the multilevel adaptive governance of a healthcare organization and its Environment, while considering influence factors, co-evolution, and the emergence of generative relationships. The proposed model (Fig. 2) thus integrates the determinants of healthcare organizations (CAS), internal actions like self-eco-organization and the adaptation process of multilevel governance, and actions directed toward the Environment involving co-evolution and generative relationships.
Adaptation?process?framework?of?an?healthcare?organization
{kind=link}
Working from our conceptual framework (Figure 2), we formulate the following proposals:
Individual Adaptation
P1.The challenges of providing care and services to migrants are found primarily at the clinical level, between the professional and the migrant person. Each stakeholder self-organizes in an individual way, and the adaptations are heterogeneous and are individually adjusted.
P2. At the individual level, maneuvering room for stakeholder flexibility and trial-and-error are favored by feedback loops throughout the process.
Adaptation by programs and spheres
P3. To go beyond the walls of the consulting room and to discontinue operating on a case-by-case basis, professionals self-eco-organize and interact with other stakeholders in the same program or sphere. In less individual and more integrated logic, they share and exploit their knowledge and know-how with stakeholders from other fields of action (operational, tactical or strategic) and from the Environment.
When healthcare organizations and the Environment enjoy favorable conditions and factors of influence (Fig. 2) (e.g. stakeholders’ autonomy, decision-making power at local level), the adaptation process can take root through multilevel governance.
When it comes to individuals and their heterogeneous adaptations, self-organization and case-by-case adaptation prevail. (P1) It is the emergence of the common point around the need to adapt that will allow individuals, through self-eco-organization, to reassemble existing forms of adaptations for migrant populations within a clinical service. (P2 and P3)
Conversely, conditions may be less favorable when influenced by various factors, such as no or few shared schemata, absence of stakeholders autonomy, top-down management, budgetary cuts, lack of personnel, centralization of power, resistance to change (especially at the strategic level), expectations from other population groups. The adaptation process will be limited in its scope and duration.
In this type of situation, operational stakeholders, especially in the clinical sphere, may remain at the case-by-case level, may not be understood by the stakeholders from other fields, and may experience limited self-eco-organization. In the absence of support from the other two fields, known adaptations will be shared and exploited at the operational level, without being able to merge collectively.
Adaptation of the healthcare organization and its environment
P4. The adaptations of the clinical and administrative spheres, and their constituting fields of action, converge through various levers of action that facilitate a coherent integration of the clinical and administrative practices between managers, administrators, and the Environment.
P5. Multilevel adaptive governance stimulates collective actions internally and with the stakeholders of the Environment. This model encourages co-evolution, the adoption of homogeneous adaptations and the emergence of new adapted practices.
P6. The stakeholders of the Environment play a fundamental role with respect to the implementation or non-implementation of favorable conditions of adaptation.
In this third group of proposals, the multilevel adaptive governance allows the identification of solution paths based on what the group of stakeholders have (P4) and where they would like to go (P5) (March, 1991). To innovate, they may use their expertise to build upon what they already know (P4 and P6).
The stakeholders in the clinical and administrative spheres put forward all of the concerns related to service adaptation. Based on envisaged or realized adaptation measures, the field of strategic action suggests a coherent view that integrates the various specificities and interests of each field. (P4, P5)
Multilevel adaptive governance becomes a space in which stakeholders can adapt through feedback loops, while considering the Environments’ stakeholders. (P5, P6)
Communication, information transfer and decision-making are at the basis of the reactivity of the organization and of the Environment with respect to the needs of migrant persons. Generative relationships are at the basis of the synergy between healthcare organizations and the Environment. (P3, P5, P6)
However, in the case of conditions unfavorable to adaptation, the lack of integration will make it more difficult to convey the concerns of the operational field to the tactical and strategic fields. If the challenge of adaptation is not prioritized, it will be forgotten despite the lack of effective solutions, since the diffusion of the adaptive strategies may only reach the tactical and strategic fields with difficulty.
At the same time, community organizations will continue to overcome the lack of coherence and of adaptation of healthcare organizations. In this case, co-evolution will signify that the healthcare organization will be less likely to homogeneously develop interventions adapted to migrant populations.
Discussion and implications for futures studies
In this study, we focused on the multilevel adaptive governance within a healthcare organization and on the sensitivity of the adaptation process to migrant persons. It remains to be determined whether the proposed model is valid in real situations where practical adaptations are proposed or realized and whether the multilevel adaptive governance framework can be applied in the long term. One way to validate the links proposed in this model would be to study, through case studies, multilevel adaptive governance in healthcare organizations that face recent, significant changes in cultural diversity.
This article attempts to contribute to the current literature that encourages professionals, researchers, and administrators to be more precise about what they expect from health services adaptation to vulnerable populations and to reconsider certain proposals regarding how and why adaptation should be implemented in a healthcare organization, through the participation of the local community networks. However, for this purpose, various studies and concrete actions opting for a systematic approach based on political are still required.