Introduction
Healthcare can be characterized as a complex adaptive system. From the cellular to sociopolitical levels, multiple “agents” and systems interact across shadowy boundaries and contribute to our concepts of health and healthcare. Nonlinear dynamics and sensitivity to initial conditions are inherent; and small changes in one part of the system, or embedded system, can change the context and outcome of another part, leading to significant variability and emergence in health outcomes (Goldberger, 1996; McDaniel et al., 2003; Plesk & Greenhalgh, 2001; Wilson et al., 2001).
If we accept this complexity conceptualization of healthcare (while recognizing doubters and the risk of fadism: e.g., Price, 2004; Reid & Notcutt, 2002), then we need to appreciate the innate unpredictability of health outcomes. We need to appreciate the limitations of healthcare management that is unduly bounded by the search for increasing data analysis and prediction models that will allow this complexity to be controlled. Rather than focusing investment on increasingly complex and costly “rational” control and decision mechanisms, we should be building the capability to cope with and indeed exploit this inherent variability and emergence (Anderson et al., 2000; Fraser & Greenhalgh, 2001; Kurtz & Snowden, 2003; Lemak & Goodrick, 2003; Plesk & Wilson, 2001).
Globally, information and communication technology (ICT) is increasingly being applied to the health system. Objectives and predicted benefits vary by stakeholder and system, but coordination, integration, safety, and efficiency are common themes (Institute of Medicine, 2000). There may be a range of views on the constituent parts or overall makeup of an ideal health knowledge management system. However, recurrent identified core features or principles that may be independent of place, time, or technology can be encapsulated in the mnemonic C.A.R.E. G.A.P.S. F.I.R.S.T.
The system should enhance every stakeholder’s “capacity to C.A.R.E.”; that is, perform their integral Clinical, Administrative, Research, and Educational healthcare functions. The system should accommodate the complex and holistic environment in which it is enmeshed, while recognizing, connecting, and enabling all the key stakeholders, primarily General practitioners, Allied health services (including hospitals), Patients and their Supports, as well as being Fast, Intuitive, Robust, Stable, and Trustworthy (Orr, 2004; Standards Australia, 2001; Standards Australia/New Zealand, 2001; Sveiby, 2001; Wyatt, 2001).
Historically, clinician-valued, cost-efficient systems that have sustainably delivered their predicted benefits have proven to be relatively elusive. A failure to recognize complexity, or a focus on trying to control the complexity of healthcare via increasing levels of data collection, analysis, and detailed “decision support” guideline or protocol creation, could explain, at least in part, this relative failure (Ash, 1997; Ash et al., 2004; Berger & Kichak, 2004; Bryant, 1998; Garg, 2005; Heeks et al., 1999; Southon et al., 1997).
The New Zealand health system is recognized as having one of the highest rates of clinical ICT enablement and integration in the world. Clinical information systems are pervasive within primary care (general practice) and the secondary care (hospital-based) systems are rapidly developing both their internal ICT enablement of clinical care and their ability to share information with primary care and other secondary care providers (Orr, 2004; Protti, 2003).
This paper reports on the implementation of an integrated series of electronic clinical health knowledge management systems in a large New Zealand District Health Board. In combination with standard project management, the core implementation team utilized an action research reflective learning approach to enhance their capability to cope with emergent issues and plan for each subsequent project stage. Aspects of this project have been reported in part elsewhere (Orr, 2004, 200b; Orr & Day, 2005; Orr et al., 2005).
However, this paper will detail the team’s emergent focus on, and evolving appreciation of, “process” issues of connectedness, competency, and control, particularly with regard to a central metaphor of crossing the “acceptance” or “concept—reality” gap (Heeks et al., 1999; Orr, 2000). The team’s journey and their evolving understanding of what was important for their journey can be understood through an appreciation of individual and group dynamics, system and complexity theories. In particular, mutual empathy for both self and others was identified as a core capability requirement to cope with the inherent ambiguity within complex systems.
Research context
Waitemata District Health Board provides publicly funded primary and secondary care to a population of 450,000. Waitemata, in association with two of its neighboring district health boards, has implemented a series of clinically focused ICT systems. The system developments that were the focus of this project included:
A single login interface from which all pa tient demographics, medical alerts, past treatment events, and investigations (blood tests, X-rays, etc.) can be viewed.
An electronic medical document reposi tory (including the migration of 250,000 historical documents).
A real-time patient tracking system for the emergency care center.
A surgical audit system.
Electronic referral status messaging and discharge summaries for primary care.
Electronic signoff of laboratory results.
Action research
Action research is an evolving concept. However, Dick (2001) observes that its name conveys its essence. Its primary goals are action or change and research or understanding, and synergy between the action and research. Action research typically involves cycles of action and critical reflection.
Action research was utilized as a methodology due to its explorative qualitative theory-building
emphasis, focus on change and learning, accommodation of researcher participation, and flexibility and responsiveness to deal with emergent issues within a complex changing system (Baskerville & Myers, 2004; Dick, 2001; Zuber-Skerritt, 2001).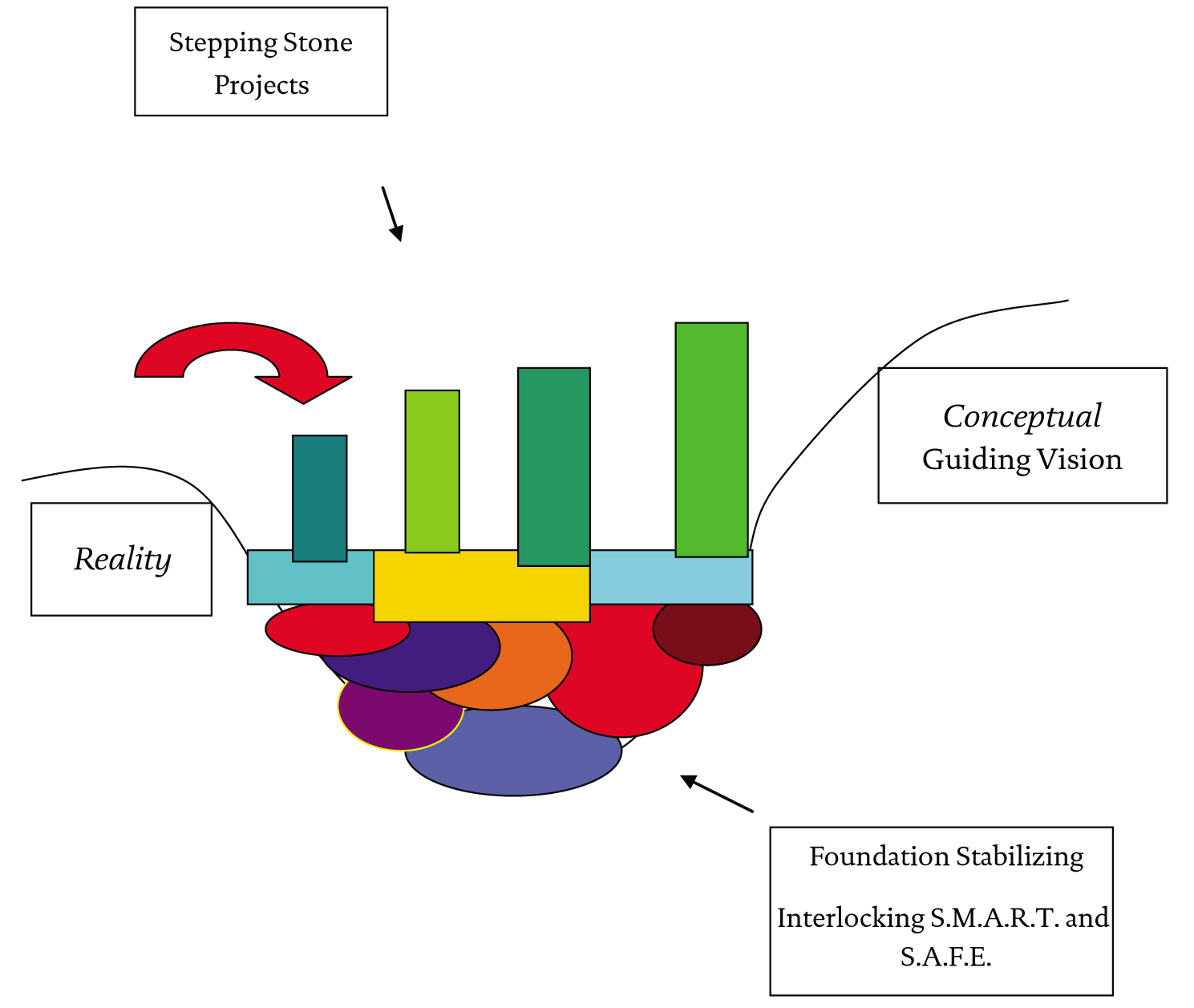{kind=link}
The research process involved an initial conceptual stage of literature review, communication with experts, and integration of personal experience. The action research stage utilized participant observation, personal and group reflection, convergent interviews, document examination, and repeated triangulation of sources seeking disconfirming evidence (Dick, 1998; Jick, 1979). The principal author had the roles of researcher, clinical director of information services, and practicing clinician (specialist psychiatrist).
Throughout its development, action research has experienced criticism of its validity, rigor, and ethics (Hope & Waterman, 2003; Meyer, 1993; Williamson & Prosser, 2002) and these issues within the context of limitations of the methodology are explored further in an additional paper related to this project (Orr et al., 2005).
Relevant findings
The “acceptance” or “concept—reality” gap
The action research cycles of action and critical reflection aimed to develop conceptual models (built on emergent key project issues and related issues) that may enhance the implementation of electronic health knowledge management systems at Waitemata. A central metaphor utilized throughout the project was that of crossing the “acceptance” or “concept—reality” gap (Figure 1). This originated as a visual representation of a common theme in a range of disciplines that as an individual or system faces a stressor or change, there may be an initial drop in functioning before a reorganization, improved resilience and capability, and return to baseline if not ideally improved function. This general theme is illustrated in such concepts as the reengineering curve, the death valley of change, crossing the quality chasm, moving through a grief process, and so on (Committee on Quality of Healthcare in America, 2001; Elrod & Tippett, 2002; Kelley & Tucci, 2001).
In an industrial reengineering process this initial drop in functioning may be acceptable if a change is expected to lead to greater productivity. However, in a healthcare system, any drop or perceived drop in functioning that may affect the system’s capacity to maintain patient safety can lead to abandonment of the new process and return to the original trusted, if flawed, process. Failure to appreciate the magnitude of the concept—reality or “acceptance” gap, with particular relation to the complex multiple enmeshed systems characteristic of healthcare, contributes to the common, at least partial, failure of ICT implementations and health system changes in general (Glouberman & Mintzberg, 1996; Heeks et al., 1999; Orr, 2000).
Evolution of gap metaphor
The original primary message of the “acceptance” gap was that you could try to jump from reality to concept in one go. However, the health ICT literature would suggest that there was a high likelihood that if your concept involved significant system change you would crash and burn. Instead, you needed to incrementalize your conceptualized vision, break the journey down into foundation and stepping stones, and recognize that each component could be further reduced again to component parts. You needed to build firm foundations of SMART (Specific, Measurable, Acceptable, Resourced, and Timelined) and SAFE (Scalable, Affordable, Flexible, and Equitable) projects, and then perhaps try some stepping-stone projects involving some process or system change, but never attempting to change too much at once (Orr, 2000, 2004).
“You’re weaving fibres together to create a beautiful rug, you’re not stacking cans in a supermarket.” (Project team member)
Reductionistic metaphors or models by their implicit nature in their attempt to clarify and simplify run the risk of losing important complexity. However, they can perform an important role in communication and act as catalysts for further individual and group understanding (Orr, 2004). A central focus of action research is to deal with the data and issues that emerge in the real system rather than be bounded by preconditions or assumptions of what those issues may be. The author had originally assumed that a major focus of the group and individual reflective sessions would be identifying a detailed technical content picture of what our conceptual vision was, our current reality, and the detailed technology stepping stones we needed to take to get there.
Instead, the focus was more on individual, group, and inter-group dynamic relationship and functioning issues, such as dealing with ambiguity, different cultures, different systems, control, competency, and connectedness. The core project team averaged only 10—12 individuals, and comprised a mixture of seconded clinicians (with various levels of project management and ICT experience) complemented by external specialist ICT contractors. However, to achieve their task the core team had to interact with and influence multiple other enmeshed systems, with the project directly affecting at least 2,500 staff in multiple teams and services, and 130 primary care practices within the district.
Simply identifying the technical content of stepping stones or a conceptual vision was not enough. Standard project management scope detailing, breakdown, and timelining aimed to fill this role and it was an important role. However, it was not just a matter of filling cans and stacking them, and the acceptance gap metaphor was repeatedly challenged with such questions as:
What was the supporting life force, pas sion, or ecosystem or “agents” that were required to build and hold it altogether?
How could you get everyone to cooperate across multiple systems with different cultures, languages, and priorities?
How should and could the building stones link, who should design, build, or own them?
Was there an optimal stone size or gap, should we have a three-dimensional model, could we identify all the stones and did we have to?
Was incrementalism always right, did it not just encourage inertia?
Was it not better sometimes just to make a leap of faith, do something radical, and force the system to change?
The reflective learning and subsequent capability development sessions helped deal with the dissonance between the simplicity of the project Gantt chart and the ambiguity, variability, and emergent issues that reflected the complexity of the system they were operating in.
The learning curve
“As move through learning curve, more focus on walking the boards than documentation… still on the rollercoaster but see things differently and know will cope.” (Project team member)
A common theme, particularly for seconded clinical team members, was an initial sense of lack of competence and lack of control, within the multiple systems they found themselves in, and a concern that they may have compensated for their perceived lack of formal technical and project management knowledge and experience with a focus on ever more detailed documentation. However, as time progressed they became more comfortable with the inherent ambiguity, and recognized that it was their intuition within, knowledge of, and ability to interact with and develop local health systems and agents that was of most value to the project. To assist people moving through this learning curve, the value of a buddy system placing people together with complementary skills was also recognized.
“The health knowledge ecosystem”
“It’s like pebbles skipping off the water… need to understand its not real for them, not the same urgency until impacting on their world.” (Project team member)
The team also faced the challenge of how each enmeshed system and agents from technical staff to clinicians were already invariably caught up with dealing with multiple changes, pressures, and requirements within their own world.
Key components or subsystems of the health knowledge “ecosystem” that emerged were the Innovation, Innovators, Implementors (both the core team and wider technical expertise), Individuals (both clinicians, patient, and administrative users), the Invironment (used to capture the concept of the associated clinical and administrative processes and wider sociopolitical holistic environment), the Investors, Informaticians, and Integrators.
Aligning the priorities of these systems was a perpetual challenge and a focus for capability development. It was also recognized that although project funding often focused on the purchase of the Innovation or software and specialist implementers, a viable health knowledge system required sustained investment in the development of all the components (Orr et al., 2005; Orr & Day, 2004).
One particular illustration of the complexity of the system was the replacement of paper lab results with electronic viewing and signoff. Significant work was involved trying to map all the subsystems that the paper lab result moved through and the actions triggered at each stage, particularly the implications if the paper triggers were removed.
Mutual empathy
In terms of capability development, reflection sessions led to the team exploring a number of areas, including the reasons health information systems fail, acceptance gaps, utility of resistance, the psychological impact of change, building networks, communication, listening, learning and linking, negotiation and dealing with difficult situations, and ambiguity.
Mutual empathy was identified as a key capability, and building on the work of Stuart and Lieberman (1993), the “empathy” mnemonic was developed to capture the key features thought important to this concept:
Emotion: How do the key stakeholders feel about an issue: their sense of control, competency, connectedness?
Motivation: What drives them: values, reason, emotion, self-interest?
Pressures: What are the pressures impacting on their behavior/decisions?
Attachments: What are the key attachments or networks for stakeholders?
Trouble: What issues trouble each stakeholder group most?
Handle: How do stakeholders cope/adapt/learn from experience/utilize supports?
You: What part do you play in each stakeholder’s conceptualization of an issue?
Acceptance gap metaphor as a projective technique
One particular focus was the need to develop a shared language, understanding, significance, and hope and priority for action between often disparate in culture but interdependent systems and agents. As time progressed (and with subsequent experience), it emerged that the acceptance gap metaphor’s major value was not in creating time-intense detailed content pictures of every specific step. Instead, it served better as a brief projective technique for groups, surfacing the assumptions and perceptions and values of those present as to what the concept, reality, perceived risks and benefits, and needed steps were, illustrating differences, but also setting the basis for moving toward that desired shared language, understanding, significance, and hope.
Emergent demand and concerns
Project management creates a very important framework to drive processes along. However, within a complex system it is difficult and of limiting utility to fix scope and timelines in concrete, and not allow for the wider and enduring systemic issues, ambiguities, emergent phenomena, challenges, and opportunities that have to be dealt with as they arise. Similarly, for the implementation team, although the project had a defined scope and timeline, as they started on their journey they uncovered all sorts of emergent demands and concerns with regard to not just how technology could facilitate the care system, but also the fundamental processes and interfaces of our systems of care. The team recognized that they were ambassadors for how ICT could empower health systems, not just for this fixed project time and scope, but for the continual process of development. They were initiating a system whereby clinicians could move from using technology on a sporadic basis for wordprocessing, email, and the internet, to integrating technology into their daily care systems and considering how it could change those systems. The team recognized the need to have clear mechanisms to capture the changes as well as processes to deal with them, but not to be sidetracked or dragged down by them.
Catalyst projects
Each component of the project could be perceived as an opportunity to get access to and attention from fully engaged preoccupied subsystems, to understand their needs, processes, and interfaces.
With all the key agents invariably busy, if anyone, but particularly clinicians, took the time to raise concerns, rather than being perceived as resistance this could be grasped as an opportunity to harness energy and enthusiasm, develop a portal, and strengthen links into their system.
Each step, project, or engaged agent can act as a catalyst toward getting a greater understanding of the complexity, needs, and attractors of interfacing systems aligning and altering if necessary one piece at a time, to build capacity for more fundamental change.
Discussion
This paper was neither an attempt at an ontological or epistemological critical analysis nor a formal prospective application of complexity theory (Phelan, 1999; Solem, 2003). Instead, it describes how a group with little academic knowledge of the language of systems or complexity theory utilized action research to build the capability to cope with the implementation of an electronic health knowledge management system within the complex health environment. The author describes how he began the journey by looking for content and ended it by focusing on process.
Mutual empathy emerged as a core capability to be identified and nourished, to help build a shared language, understanding, significance, and hope, and thrive within a complex environment of inherent ambiguity and variability, and issues of control, competency and connectedness.
The author as psychiatrist repeatedly questioned how much this emergent focus on dynamic and complex system issues was a function of his own selective abstraction or cognitive filters, or his influence on the group as participant observer. However, this focus can be traced to the intertwined origins of action research and group dynamics, with Kurt Lewin being considered a central originator of both, and both being born out of a central appreciation of iterative reflection, systems, and relationships and the need to deal with the emergent variability of the real world (Lewin, 1948).
With action research’s enmeshed links with group dynamics, the hope is that it can get the group from “forming” to “performing” while minimizing the negative impact of “storming” and eventual “mourning” (Tuckman, 2001; Tuckman & Jensen, 1977).
The concept of a health knowledge management system utilized in this paper aims to move away from the inherent focus on technology when discussing such issues as the “electronic patient record” and highlight the essential importance of taking a wider holistic view. This is a view that recognizes complexity and the need to develop the required sustaining systems, interfaces, and empathy (between Innovators, Innovation, Implementors, Individuals, Invironment, Investors, Informaticians, and Integrators) and a culture that respects, values, and protects the creation, acquisition, and sharing of health information.
Project management, action research, complexity, and the development of critically reflective practitioners
There is an increasing recognition within the formal project management literature of a need to re-examine some of its fundamental tenets if it is to cope and add value in an increasingly complex environment: a need to develop critical reflective practitioners with the capability to embrace complexity and emergence and thrive within an environment where all outcomes and interactions cannot be readily predicted or controlled.
Winter and Smith (2006), reporting on the UK “rethinking project management” research network, identify five key directions for future project management research. These key directions emphasize the need to recognize the complexity of projects, the inherent social process, a move in focus from product creation to value creation, a broader conceptualization of projects that recognizes and can adapt to multiple objectives or fuzzy or nonpredefined emergent objectives, and a shift in practitioner development focus from one that produces trained technicians toward facilitating the development of reflective practitioners. Similarly, Jafaari (2003) concludes that project management requires further research and development of a “creative-reflective” model if it is to avoid irrelevance in an increasingly complex world. This project echoed the importance of many of these issues.
Wilson et al. (2001) suggest some principles to facilitate decision making in the “complex zone.” These are using intuition, experimenting, minimum specification, chunking, using metaphors, and asking provocative questions. These principles or techniques evolved within the team as a natural consequence of the action research reflective learning process, adding some empirical support to action research’s perceived synergic utility with traditional project management processes within a complex environment.
Snowden’s “three ages” of knowledge management
Snowden (2002) posits that we are entering a third age of knowledge management. The first age was correlated with the dominance of business process reengineering and focused on the computerization of key processes and the structure and flow of information to decision makers. The first age failed to value or recognize the importance of experience, apprenticeship, or collective knowledge.
The second age beginning circa 1995 was driven by the SECI (Socialization, Externalization, Combination, Internalization) model (Nonaka & Takeuchi, 1995), with a focus on converting knowledge from tacit to explicit forms. Snowden (2002) notes that the concept of tacit and explicit knowledge was not new (Polanyi, 1974), and had and continues to have value. However, Snowden (2002) argues that a major failing of the second age was a dualistic rather than dialectical interpretation of the tacit-explicit concept and in particular the SECI model. Snowden comments that Nonaka (Nonaka & Konno, 1998) later went on to attempt to clarify and emphasize the dialectic and holistic intent of the original model. However, the widespread dualistic misinterpretation saw knowledge frequently viewed as a “thing” that could and should be separated from its origin and context, codified, stored, valued, and traded; tacit and explicit as two opposites rather than integral parts of the same whole.
Stacey (2001) contends that knowledge is not a “thing” that can be stored or managed but a dynamic relational process. Snowden (2002), commenting on Stacey (2001), argues that knowledge can be perceived as a “thing” but also paradoxically as a “flow,” and our understanding and knowledge are enriched by synergically exploring both perspectives.
Snowden (2002) argues that in the “third generation of KM” we need to further evolve our knowledge management capability, so that we are no longer primarily focusing on content management where knowledge is perceived as a “thing,” but shift our paradigm to also appreciate knowledge as a “flow” where context and narrative are inherent.
The “third age” value of traditional healthcare knowledge processes
Healthcare is globally considered one of the last great challenges, and increasing priorities for information and communication technology (ICT) facilitated process reengineering. ICT can certainly play a role in helping healthcare better manage knowledge to facilitate more effective integrated care. However, there is a need for ICT professionals entering the healthcare area not to make the same mistakes as other industries. They need to recognize the “third age” value of traditional healthcare knowledge processes and avoid regressing healthcare back to live through the negative aspects of Snowden’s first and second ages. Context, story telling, apprenticeship, fellowship, professional ethics, community, and collective knowledge have been central to traditional models of clinical development and practice. ICT should seek to value and enhance these important traditional processes.
A “third age” health knowledge management system
Healthcare requires critically reflective practitioners who can cope in real time with the complex ambiguity they often face. ICT can facilitate creating a context or supporting ecosystem for healthcare workers to facilitate the development and exercise of this critical reflectiveness; a context for collaboration with their stakeholder communities and connection with their supporting resources; a context that can provide timely knowledge and coordination and facilitate the self-organization and management of knowledge (Snowden, 2002).
Systems designed to facilitate the control or predictions of risk in the health environment certainly have a role. However, systems designed to control risk by controlling clinicians via the application of increasing levels of rules that do not take into account the complex time-pressured environment in which clinicians operate have frequently met with failure. As well as being switched off due to their sheer lack of utility, they can also potentially lead to increased risk due to their capacity to disempower the clinician’s sense of ownership and responsibility and in-the-moment critical reflectiveness. There is a need to avoid autopilot systems that result in the driver falling asleep at the wheel or becoming deskilled to the point where they can no longer cope with the complex ambiguity inherent in their work. Systems need to synergically enhance and build on, rather than try to replace, clinicians’ professional ethical training and core critical reflectiveness.
Attempting to control or predict the risk of an undesirable outcome in a complex environment by introducing ever-increasing levels of rules or barriers, based on a retrospective analysis of a past undesirable outcome, is fraught with limitations. Such an analysis may certainly assist an understanding and system improvement. However, this is with the caveat that the reviewers appreciate the role of retrospective coherence, and that although it may appear to make perfect logical sense as to what factors contributed to an adverse outcome or pattern, these factors in a complex environment may have resulted in several different outcomes or patterns (Snowden, 2005).
In a complex environment it is important to consider not just how the barriers to the conditions or patterns associated with bad outcomes can be increased, but also to enhance and develop the attractors associated with good outcomes (Snowden, 2005).
Growing the right thing
The central focus for the systems implemented in this project were not to control clinician behavior but to create a context that enhanced the frequency of patterns known to be associated with good patient care outcomes; namely, timely access to appropriate information and communication with other caregivers. Throughout the design and implementation process there was always (and with ongoing developments there continues to be) a focus on not just how you may stop people doing undesired things, but how do you help users do the right thing.
The primacy of the core clinician—individual patient relationship
Though there has been a shift to a population health focus that may consider an individual’s needs within the context of a community’s needs, and associated costs and opportunity costs, traditionally the predominant culture, values, or attractors for clinicians, from basic training to ongoing professional development, have focused on the primacy of the core clinician—individual patient relationship. There is an increasing capacity for electronic technology developments to affect that core relationship via the introduction of decision support or guidelines. As noted previously, such decision support or guidance has the potential to be of significant value. Unfortunately, guidelines are often experienced as inflexible mandated protocol, a linear solution in a complex nonlinear environment that fails to recognize and accommodate complexity, variability, and emergence. Electronic health knowledge systems that seek to provide guidance need to embrace their key function of acting as potential catalysts for the wider ecosystem to review, align, and develop their associated context, processes, values, and key relationships. The technology and content can be borrowed or purchased, but will still need the associated professionalism, processes, and relationships to deal with ambiguity, and balance risks and benefits, costs and opportunity costs (Grol et al., 1998; Rousseau et al., 2003; Shiffmann et al., 1999).
Informing and connecting rather than controlling and changing
The project developments discussed in this paper, in keeping with the majority of developments in New Zealand to date, are focused on enhancing the core clinician—patient interface, informing and connecting rather than controlling or significantly changing traditional clinical processes or systems. These developments are designed to provide a context to network the knowledge of key stakeholders so that better questions can be formulated, rather than the focus being on providing mandated answers. This focus to date may have contributed to the relative success of clinical ICT diffusion in New Zealand, while also incrementally building the capability for more fundamental positive change. This includes the ongoing development of electronic guidelines and decision support that recognize and embrace complexity and chronicity as well as individual and group needs and values.
Health knowledge system implementation investments are typically focused on the Innovation or piece of software and the Implementors. This project and ongoing developments have highlighted that a sustainable health knowledge system requires the need to invest not just in the Innovation and Implementors, but in a long-term developmental relationship with the wider ecosystem of Innovators, Invironment, Individuals, Investors, Integrators, and Informaticians. Investments in each area can grow and interconnect and support each other, increasing the capacity for all areas to progress. For the implementation team, core ethical values of professionalism, critical reflectiveness, and mutual empathy for others, rather than fixed rules, were central to the team’s capacity to operate in a complex, ambiguous environment. Similarly with ongoing developments, core values, reflectiveness, and professionalism continue to play a central role, as we strive to create an environment that respects, values, and protects health knowledge.